Cardiothoracic surgery post operative ICU management |
|
Summary
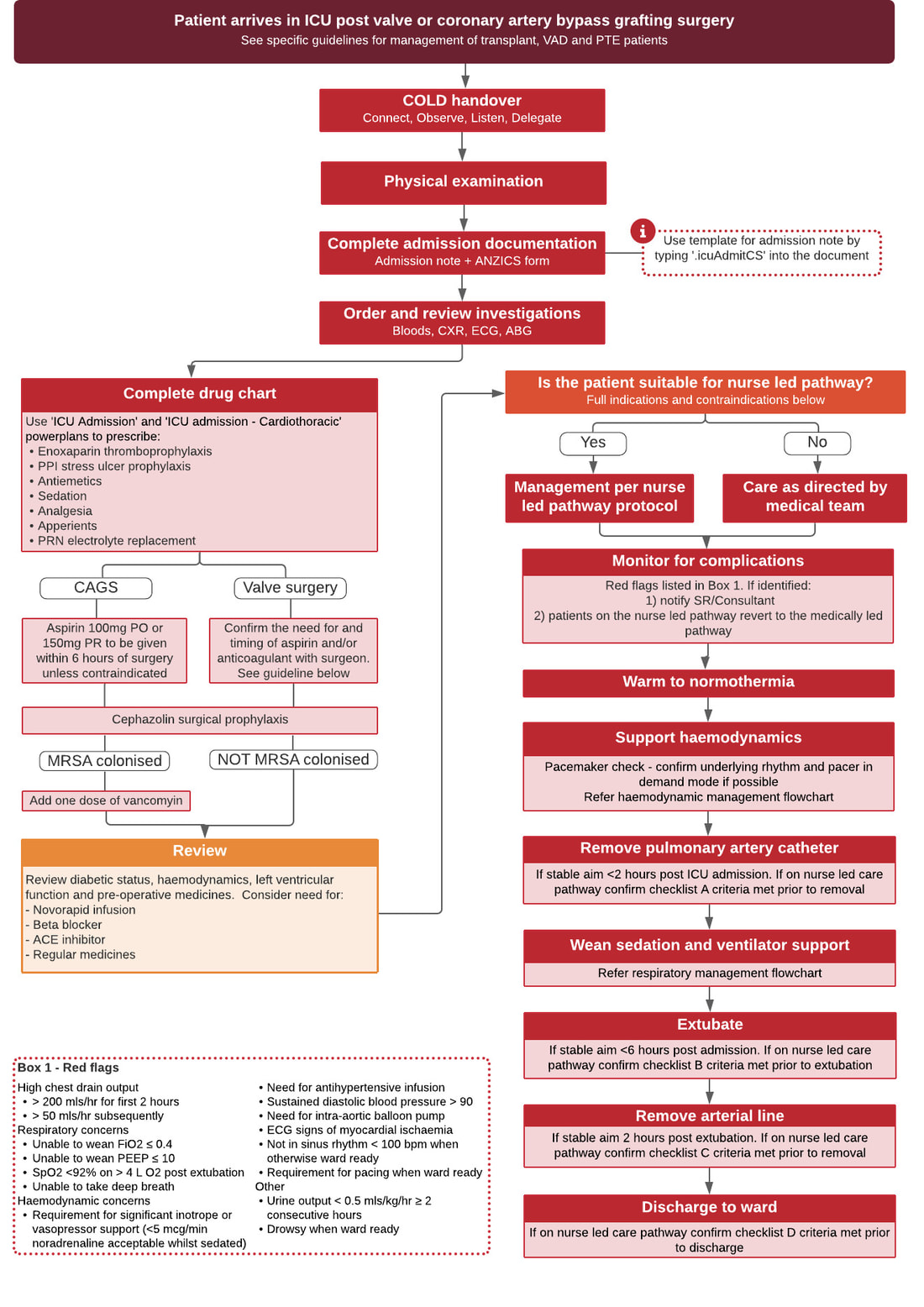
Table of Contents |
Admission Documentation
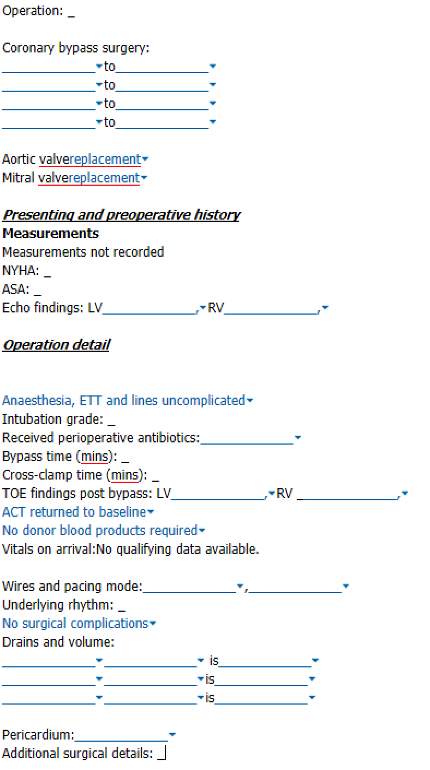
When a patient arrives in ICU from the operating theatre after cardiothoracic surgery the anaesthesiology and cardiothoracic teams will provide a verbal handover to the ICU team
- At this point in time, some of the clinical information provided in this verbal handover may not yet be documented elsewhere
- To ensure no clinical information is lost, it is important that the doctor completing the ICU admission note use a structured format
- A standard template (with dropdown boxes for ease of completion) is available for this purpose and should be used for all admissions to ICU post valve or coronary artery grafting surgery
- The template can be activated by typing ‘.icuAdmitCS’ into the admission note and is shown below
- An ANZICS data collection form should also be completed for all patients admitted to ICU
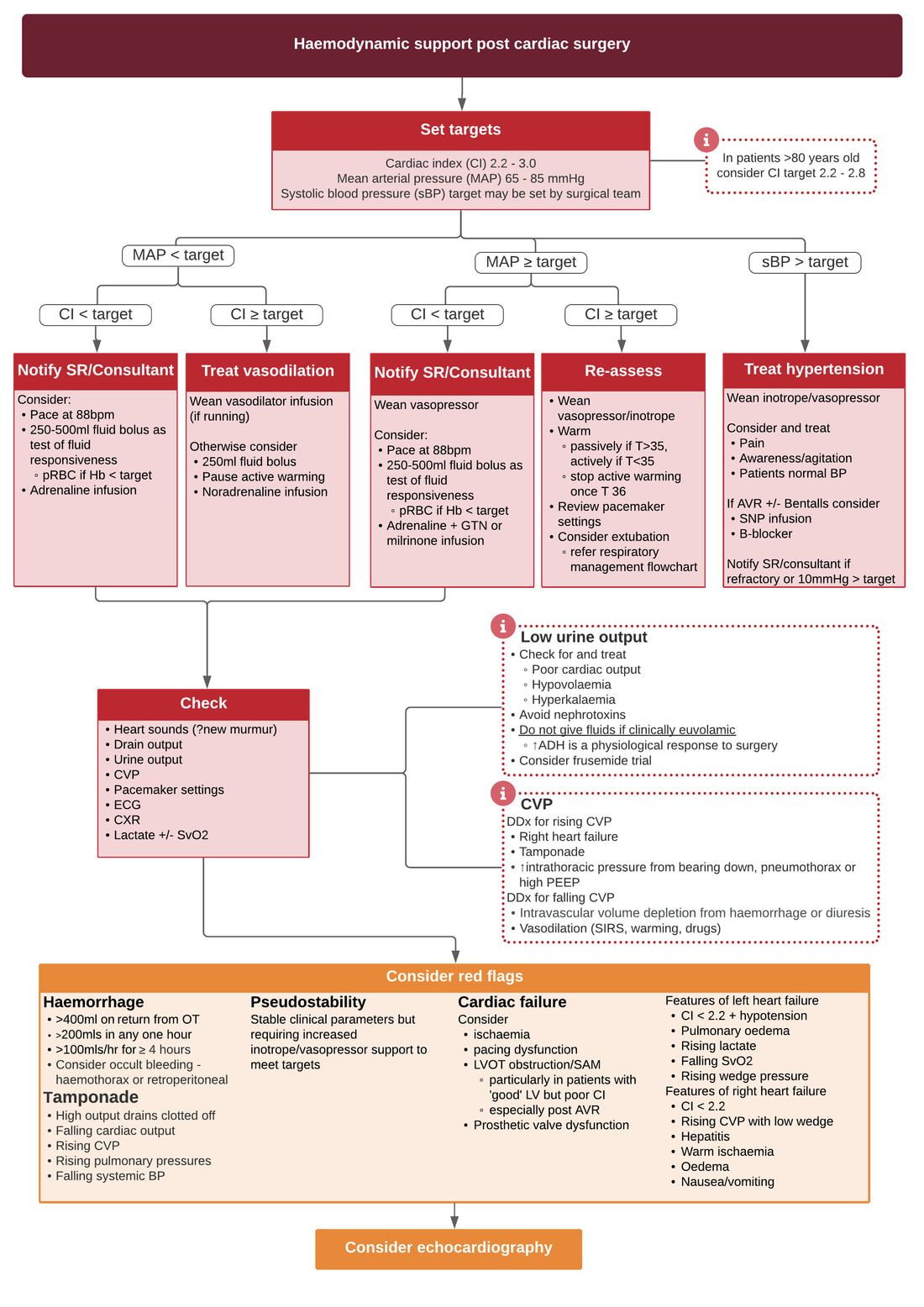
Haemodynamic Management
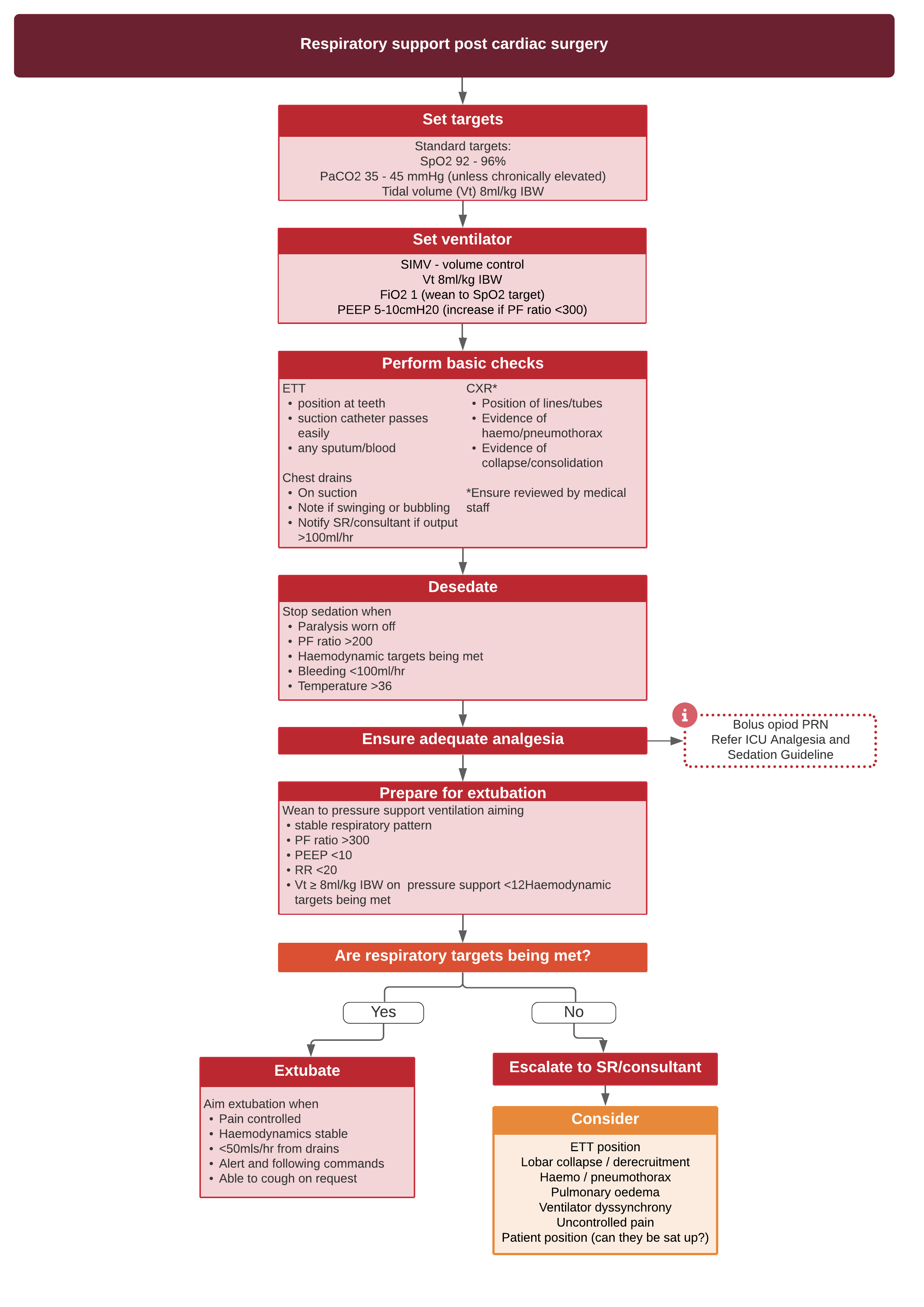
Respiratory Managment
Treatment of atrial fibrillation (AF) post cardiothoracic surgery
- It is common for patients to develop AF (with or without rapid ventricular response) after cardiac surgery.
- In patients who are asymptomatic, AF is frequently self-limiting – up to 30% will spontaneously revert to sinus rhythm within 2 hours, and up to 80% will do so within 24 hours. (5)
- As a result, in monitored and haemodynamically stable patients with post-operative AF, it is reasonable to exclude electrolyte and volume state abnormalities before considering more aggressive therapies.
- If treatment is required
- For patients without adverse signs electrolyte replacement and beta blocker therapy is recommended (6)
- If adverse signs are present, but the patient is stable, an amiodarone load of 300mg over half to one hour plus an infusion of amiodarone should be commenced
- Where the patient is haemodynamically unstable, cardioversion is required
- Digoxin is often not useful also due to the high adrenergic tone after cardiac surgery.
Management of cardiac arrest ofd life-threatening bleeding
It is of critical importance that all clinicians caring for patients post cardiac surgery are aware that:
- The management of cardiac arrest in patients <14 days post cardiac surgery differs from standard advanced life support algorithms
- In the event of cardiac arrest and/or life threatening bleeding it is occasionally necessary to perform a resternotomy
- Detailed guidance and protocols can be found in the Management of cardiac arrest post cardiac surgery in the ICU clinical practice guideline
Medications to prescribe post cardiac surgery
It is essential to review and rationalise a patient’s drug chart on admission to ICU. During business hours this can often be done in conjunction with the ICU pharmacist, in accordance with the ICU partnered Post Op CTHR Medication Charting Procedure. Guidance on prescribing post cardiac surgery can be found below.
Thromboprophylaxis
All patients should have thromboprophylaxis commenced on the day after surgery (if not contraindicated).
Standard prescription:
Further guidance can be found in the thromboprophylaxis guideline - sections 7.4 and 7.5 contain information about enoxaparin dosing adjustments.
When pharmacological thromboprophylaxis is contraindicated mechanical aids should be considered.
Standard prescription:
- enoxaparin 40mg subcut daily (if eGFR >30mL/min and weight 50kg-120kg)
- Dose reductions are required for low body weight and renal impairment
- Dose increases should be if weight >120kg
Further guidance can be found in the thromboprophylaxis guideline - sections 7.4 and 7.5 contain information about enoxaparin dosing adjustments.
When pharmacological thromboprophylaxis is contraindicated mechanical aids should be considered.
Stress Ulcer Prophylaxis
Proton pump inhibitors are routinely prescribed for intubated patients as stress ulcer prophylaxis. Once the patient is extubated and tolerating enteral nutrition, IV therapy should be switched to an oral formulation. Stress ulcer prophylaxis should be continued for one-month post-surgery.
Standard prescription:
Standard prescription:
- pantoprazole 40mg IV daily
- once enteral administration possible switch to esomprazole 40mg NG daily or pantoprazole 40mg PO daily